Wernicke’s Encephalopathy represents a severe, acute neuropsychiatric emergency that demands rapid clinical recognition. Missing this presentation can result in permanent neurological deficits or death. Understanding the precise metabolic underpinnings of this condition ensures that medical professionals can intervene safely and effectively.
Defining Wernicke’s Encephalopathy
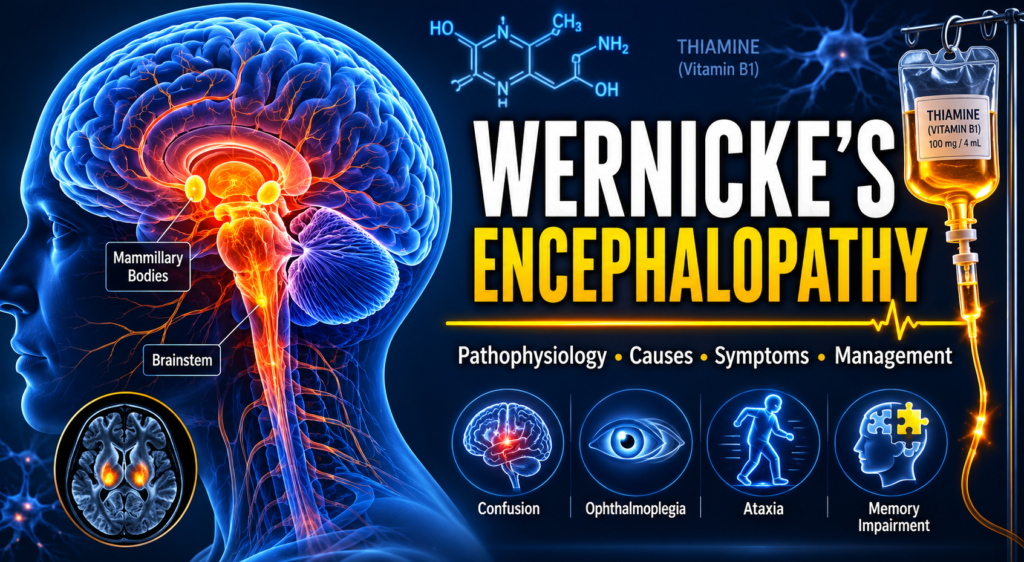
Wernicke’s Encephalopathy is an acute, life-threatening neuropsychiatric condition born from a severe systemic deficiency of Vitamin B1, commonly known as thiamine. Crucially, this metabolic crisis is highly reversible if clinicians identify the symptoms early and deliver immediate treatment.
When the human body experiences an extended depletion of thiamine, metabolic pathways in the brain fail. Consequently, cellular damage accumulates rapidly within vulnerable cerebral structures like the mamillary bodies and brainstem nuclei. If the condition remains untreated, the acute state can quickly transition into a chronic, permanent amnestic disorder. Early identification remains the single most important factor in saving a patient’s cognitive and neurological function.
Primary Etiologies and Vulnerable Patient Populations
Thiamine deficiency occurs due to poor nutritional intake, inadequate gastrointestinal absorption, or excessive metabolic loss. While many associate this metabolic crisis with chronic alcohol use, it actually develops across a diverse spectrum of clinical conditions.
Chronic Alcoholism
Chronic alcohol use disorder represents the most common cause encountered in emergency medicine. Individuals with this condition frequently experience poor dietary intake of essential vitamins. Furthermore, chronic ethanol consumption actively impairs the gastrointestinal absorption of thiamine in the small intestine while decreasing hepatic thiamine storage. This dual mechanism of poor intake and reduced absorption dramatically accelerates the onset of neural depletion.
Non-Alcoholic Nutritional Deficiencies
Wernicke’s Encephalopathy can easily emerge in individuals who do not consume alcohol. Medical professionals must maintain a high index of suspicion when evaluating patients with severe nutritional disturbances, including:
-
Severe Eating Disorders: Conditions like anorexia nervosa drastically reduce the baseline ingestion of vital nutrients.
-
Gestational Complications: Hyperemesis gravidarum causes prolonged, severe vomiting during pregnancy, quickly exhausting maternal thiamine stores.
-
Surgical Interventions: Gastrointestinal surgeries, such as bariatric procedures or bowel resections, alter the anatomical pathways required for micronutrient absorption.
-
Extended Deprivation States: Prolonged fasting, severe hunger strikes, or systemic starvation deplete standard hepatic reserves within weeks.
-
Chronic and Systemic Diseases: Systemic malignancies, advanced HIV/AIDS, and organ transplantation place immense metabolic demands on the body while limiting nutrient retention.
-
Renal Therapies: Both hemodialysis and peritoneal dialysis can inadvertently clear water-soluble vitamins like thiamine directly from the bloodstream.
The Classic Symptom Triad: Understanding the “CAN” Mnemonic
The clinical diagnosis relies traditionally on a classic triad of clinical features. This hallmark presentation can be easily remembered using the simple medical mnemonic CAN. Think of a “can of beer” to anchor this memory tool during high-pressure emergency assessments.
1. C is for Confusion (Encephalopathy)
Confusion represents the core encephalopathic component of the disease process. Patients present with profound disorientation regarding time, place, or identity. They display a distinct mental indifference, apathy, and extreme lethargy. During physical examinations, affected individuals exhibit severe inattentiveness, and their speech may appear sluggish or completely incoherent.
2. A is for Ataxia (Gait and Stance Impairments)
Ataxia alters a patient’s physical stability and locomotive coordination. This symptom develops due to a combination of central and peripheral nerve damage. Peripheral polyneuropathy reduces baseline sensation in the lower extremities, while cerebellar involvement disrupts central motor planning and balance.
Consequently, patients exhibit a classic wide-based gait. They move with slow, short, hesitant steps because they feel unstable on their feet. In advanced scenarios, the individual may lose the ability to stand or sit independently.
3. N is for Nystagmus (Ocular Motor Dysfunction)
Nystagmus is the most common sign of ocular motor failure on examination, but it reflects a broader spectrum of ocular movement pathologies. The deficiency injures the delicate nuclei of cranial nerves III, IV, and VI, producing several distinct visual disturbances:
-
Abducens Nerve Failure: Lateral rectus palsy develops frequently and typically impacts both eyes symmetrically, restricting outward eye movement.
-
Gaze Paralysis: Conjugate gaze palsies prevent the eyes from moving together smoothly in horizontal or vertical planes.
-
Pupillary Disturbances: Affected individuals may display sluggish pupillary reflexes when exposed to light vectors.
-
Anisocoria: The physical examination may reveal unequal pupil sizes between the left and right eyes.
Additional Clinical Indicators
Beyond the primary triad, advanced stages of thiamine depletion can cause deeper systemic failure. Patients can decline into an unarousable coma. Furthermore, the loss of autonomic regulation can cause profound hypotension and hypothermia as hypothalamic function becomes compromised.
Molecular Pathophysiology: Why Thiamine Matters
To understand why these symptoms occur, one must evaluate the role of Vitamin B1 within cerebral metabolism. Thiamine serves as an obligate cofactor for several key enzymes inside cellular energy pathways.
Specifically, three mandatory enzymes require thiamine to process carbohydrates and generate cellular energy:
-
Transketolase: This enzyme drives the pentose phosphate pathway to generate cellular resources and maintain myelin sheaths.
-
Alpha-Ketoglutarate Dehydrogenase: This complex sustains the citric acid (Krebs) cycle to generate cellular adenosine triphosphate (ATP).
-
Pyruvate Dehydrogenase: This bridge enzyme links the products of glycolysis directly into mitochondrial respiration.
If thiamine is absent, these critical enzymatic machines turn completely inactive. Consequently, the brain experiences a localized failure in energy metabolism. Because vulnerable structures like the mamillary bodies and brainstem nuclei consume high levels of energy, these specific regions experience rapid cellular injury, swelling, and petechial hemorrhages when metabolic pathways shut down.
Emergency Treatment Protocol: The Golden Rule of Glucose
The management of Wernicke’s Encephalopathy relies on the rapid, parenteral replacement of Vitamin B1. Clinicians must deliver high doses of intravenous (IV) thiamine immediately upon suspecting the condition. Typically, therapy involves administering higher amounts during the initial days, followed by lower maintenance doses to replenish systemic reserves completely.
The Absolute Contraindication
Medical professionals must remember one absolute rule during resuscitations: never administer glucose solutions before giving thiamine. This ordering error can cause catastrophic, irreversible neurological destruction.
If a clinician administers an IV fluid bag containing dextrose or glucose to a thiamine-deficient patient, the sugar influx forces cells to undergo glycolysis. This sudden metabolic demand rapidly consumes the tiny remaining scrap of active thiamine in the brain. Consequently, the vital enzymes stop functioning entirely, forcing immediate metabolic collapse and accelerating cellular death within the brainstem. Therefore, you must always ensure that the thiamine infusion is running before any carbohydrate source enters the patient’s bloodstream.
Long-Term Consequences: Progression to Korsakoff’s Syndrome
When Wernicke’s Encephalopathy is ignored or treated improperly, it can progress directly into a long-term condition known as Korsakoff’s Syndrome. This represents the chronic, lasting stage of the original thiamine deficiency.
Unlike the acute phase, Korsakoff’s Syndrome is frequently irreversible. The clinical presentation shifts from acute confusion toward profound structural memory deficits. Affected individuals winter severe anterograde amnesia, which eliminates their ability to form new memories.
Additionally, these patients demonstrate confabulation. They unconsciously invent detailed, fabricated stories to fill the blank spaces in their memory fabric. Because the patient genuinely believes these false memories, they are not intentionally lying. This permanent memory damage leaves individuals unable to live independently. Protecting the initial acute patient with immediate thiamine delivery remains the ultimate defensive strategy against permanent cognitive disability.